
It is the second week of user acceptance testing for a new speech-to-text dictation system in an NHS trust. The system is one of more than a dozen digital products this trust’s Clinical Safety Officer is currently responsible for. This week, the dictation system is the one on her desk. She is reviewing a sample of the AI’s transcriptions against what was actually spoken in the consultation room.
She finds it on the eighty-third dictation. A consultant cardiologist had said, into the microphone: “commence digoxin two hundred and fifty micrograms once daily.” The system had transcribed: “commence digoxin two hundred and fifty milligrams once daily.”
The dose of digoxin in an adult is 125 to 250 micrograms after the initial dose. Two hundred and fifty milligrams is a thousand times that. A single dose would kill within hours.
The system was three weeks from go-live across nine clinical pathways. Now it isn’t.
What the Role exists to do
A Clinical Safety Officer is the senior clinician an NHS organisation, or a health tech company, relies on to make sure that the software involved in clinical decisions does not harm patients. And to prove, when something does go wrong, that the harm was foreseen and mitigated as far as reasonable practice allows.
The role exists because software now sits inside almost every clinical pathway. Decisions about diagnosis, triage, medication and escalation are increasingly shaped or made by digital systems. UK regulation requires a named senior clinician to own the safety risk these systems introduce.
Two standards govern the work. DCB 0129 applies to organisations that manufacture clinical software. DCB 0160 applies to organisations that deploy it. Any NHS body deploying digital systems that affect clinical decisions is accountable under DCB 0160. This includes EPRs, AI ambient scribes, patient administration systems, e-prescribing platforms, clinical decision support tools, maternity information systems, and remote monitoring services. The companies that built those systems are accountable under DCB 0129. Both standards require a named Clinical Safety Officer.
That is what gives the role its weight. A trust running a digital system without a named Clinical Safety Officer is, in regulatory terms, running it unsafely.
A Typical Week
Monday morning the CSO chairs the hazard log review for the EPR programme. Eleven hazards on the open list. Three can be closed because their mitigations have shipped in the latest release. Two she has to escalate to the Chief Clinical Information Officer because the testing evidence is incomplete and the next deployment is in twelve days.
Tuesday she is drafting the clinical safety case for an AI ambient scribe pilot before it expands from outpatients into emergency medicine. Her job is to write, in language that a board member, a senior engineer and an MHRA auditor can all read, why the model’s accuracy on natural clinical speech is acceptable in this specific context, and the conditions under which it would stop being.
Wednesday she chairs a post-incident review on the e-prescribing module. A GP in primary care reported a near-miss where the medication reconciliation step misclassified a drug interaction. She has ninety minutes with three engineers and a UX designer to map the contributing factors and agree what changes before the next sprint.
Thursday morning is the divisional patient safety committee. She presents two themes from the last quarter’s digital incident data and is asked to come back next month with a deeper read on one of them. Thursday afternoon she sits on the procurement panel reviewing three shortlisted vendors for the trust’s new clinical decision support tool. The contract is worth four million pounds. Whatever they choose, she will be writing the safety case before it touches a patient.
Friday is deep work. Supplier safety cases to read. The quarterly Board assurance report to write.
The data, anchored in real job packs
Eleven Clinical Safety roles are open across the NHS right now. Ten of them were posted in the last seven days. This market moves quickly, and openings rarely sit unfilled.
Across the wider Career Co-Pilot dataset, 160 Clinical Safety roles have been tracked over the last two years, spanning 47 distinct job titles. The concentration sits at Band 7 and 8a. These are the bands a doctor is most likely to be a credible candidate for.
But the more useful finding sits underneath the numbers. We separated every job pack into two halves: the job description (what the role does) and the person specification (what the candidate is required to know). Then we searched both halves for the technical frameworks doctors assume gate these roles. What emerges is that “Clinical Safety” is not one hiring track. Within the roles that doctors actually compete for, it is two.
Track 1. Patient Safety roles.
Patient Safety Manager. Patient Safety Officer. Quality and Patient Safety Manager. Governance Manager Clinical Quality & Safety. These dominate the dataset. The job descriptions in these packs talk about PSIRF, incident investigation, root cause analysis, governance committees. But the person specifications rarely require knowledge of these frameworks as essential. PSIRF Implementation appears in eight job descriptions but only three person specs. Root Cause Analysis appears in three descriptions but zero person specs. Datix appears in five descriptions but only one spec. Trusts describe the work using the frameworks. They hire on clinical background plus transferable skills like stakeholder management, communication, leadership and incident-investigation experience. They train people on the frameworks once they are in the role.
Track 2. Digital Clinical Safety Officer roles.
In our dataset these appear under titles like Digital Clinical Informatics Safety Specialist, EPR Clinical Safety Officer, and the broader “Clinical Safety Officer” title when the postholder sits inside a digital team. A current real example is The Christie’s Digital Clinical Safety and Governance Officer role. The titles can be misleading though. The work itself spans the trust’s entire digital footprint. EPRs and electronic prescribing modules sit alongside AI ambient scribes, patient administration system replacements, clinical decision support tools, remote monitoring services, and the procurement of new SaaS systems before they touch a patient. The title may say “EPR”, but the remit rarely stops there.
Here the gate is different from Track 1. DCB 0129 and DCB 0160 knowledge appears as essential in the person spec, not just descriptive in the job description. The NHS Clinical Safety Officer qualification is essential, not desirable. The Christie role lists expert knowledge of the DCB 0129 and DCB 0160 standards as essential, alongside training in digital healthcare or clinical informatics. If this is the track you want, the qualification is a gate. You complete it before you apply, not during the process.
One thing both tracks share, and which catches many doctors off guard at the application stage: the wording of essential criteria almost always presumes a nursing or AHP background. “Qualified nurse or allied health professional with current NMC or HCPC registration” is a typical essential line. Doctors are eligible under broader phrasings like “qualified clinician” or “registered clinical professional”, but you are rarely the assumed candidate. A doctor applying needs to actively translate their clinical governance, M&M, audit and incident-investigation experience into the language the spec uses, or risk being filtered out at sift.
Three other tracks exist under the Clinical Safety umbrella, which this post does not focus on. Medicines Safety roles (Medication Safety Officer, Medicines Safety Pharmacy Technician, and similar titles) are pharmacy-rooted and typically require GPhC registration. Occupational Health and Safety roles like Health and Safety Manager, Fire Safety Manager, and Health Safety and Risk Lead require formal H&S qualifications and IOSH membership rather than clinical experience. The Patient Safety Partner role is a paid lay appointment specifically for people with lived experience of NHS care, not for active clinicians. These are real, well-defined career paths. They are simply not where most doctors land.
What translates from medicine, and what doesn’t
The temptation when reading a Clinical Safety job pack as a doctor is to look at the unfamiliar specialist terms (DCB 0129, PSIRF, Datix) and decide you are not the candidate. The opposite is closer to the truth. We pulled every essential and desirable skill from the 160 Clinical Safety job packs in the dataset. The top of that distribution is a list of competencies any UK-trained doctor exercises every working day. Here are the skills the job packs ask for, ranked by how often they appear, mapped to what you already do in clinic.
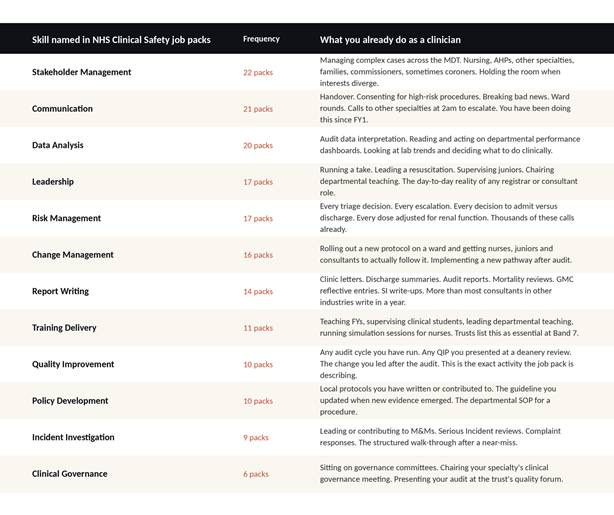
Twelve of the top sixteen skills NHS Clinical Safety employers ask for in writing are activities you do as a doctor without thinking of them as transferable. The work of moving into Clinical Safety is, in significant part, the work of renaming what you already do so that an NHS recruitment manager can score it against their criteria sheet.
What does not translate, and where you will have to do real building, is three things.
First, the vocabulary of software development. Sprints, backlogs, releases, environments, regression testing. Engineers and product managers share this language with each other and expect their CSO to follow it. You do not need to write code. You do need to know what a sprint is, why a release is not the same as a deployment, and what a regression suite is meant to do.
Second, regulatory literacy. DCB 0129 and DCB 0160 are not long documents but they are precise ones, and the language is unlike clinical practice. Read them. Then read them again.
Third, the discipline of writing for two audiences at once: engineers who want concrete acceptance criteria, and clinicians who want clinical reasoning explained in clinical terms. Get reasonable at this and you become very hard to replace.
The Transition Cost: Real Numbers
The realistic prep time before you start applying is two to four months if you can focus on it, six months if you are working clinically full time and studying in your evenings. The single most-useful action is to complete the NHS Digital Clinical Safety Officer training, both Foundation and Practitioner level. It is free, online, and gives you the vocabulary the senior CSOs interviewing you will use. For Digital CSO roles, that training is essential, not desirable. Finish it before you apply.
On money. Most Patient Safety roles for clinicians sit at Band 7 (around £47,810 to £54,710 in current AfC rates) or Band 8a (around £55,690 to £62,682). Digital CSO roles tend to start at Band 8a. A doctor moving from a clinical training programme or an early consultant post will usually take a pay cut on entry. The trajectory bends back up faster than most people expect. Most doctors I have spoken to who made this move were at consultant-equivalent pay within twenty-four to thirty-six months. The ones who moved into industry rather than NHS roles often got there sooner.
Time from your first application to your first offer ranges from six weeks to six months. The variation is mostly about how clearly you can frame your existing clinical experience in the language the person spec uses.
Where the role goes next: Progression and Exits
The Band 7 entry point is not where most doctors stop. Looking across the 160 roles in our dataset, Band 8a is the most-populated band in the entire domain. More populated than Band 7. That tells you something useful. The role does not cap at “senior specialist”. The progression is real, and it is documented in the actual hiring market.
The vertical path inside Clinical Safety, for a doctor who entered at Band 7, looks like this. Eighteen to thirty months in, you are competitive for Band 8a titles like Lead Clinical Safety Officer, Senior Patient Safety Lead, EPR Clinical Safety Officer, Head of Quality and Patient Safety, or Digital Clinical Informatics Safety Specialist (UCLH posts this one). The work changes at this step. You are now leading a function, not contributing to one. You line manage a small team, you chair governance sub-committees, and you are accountable to executive leadership for the safety case across multiple programmes.
Past Band 8a, the route bifurcates. Band 8b head-of-function roles exist in larger trusts and in the private sector. East Sussex Healthcare’s Head of Safety, Effectiveness and Compliance is the dataset’s clearest NHS example. HCA Healthcare UK posted a Band 8b Clinical Safety Officer. Elysium Healthcare posted a Band 8b Patient Safety Manager. These are senior leadership roles, not technical specialist roles. The work is organisational. Setting strategy. Presenting to boards. Owning a multi-team function.
The horizontal exits are where the most interesting careers go. Three routes show up consistently in the data. Inside the NHS, Clinical Safety experience is credible foundation for the Chief Clinical Information Officer track, which is a Director-level board role in most trusts. At the system level, Integrated Care Boards hire safety leads (NHS Greater Manchester appears in our dataset), and NHS England’s Patient Safety and Clinical Risk teams recruit from this pool. Outside the NHS, the larger health tech companies are hiring full-time Clinical Safety Officers, and the most senior of those roles (VP of Clinical Safety, or Chief Medical Officer at digital health companies) sit on compensation curves that the NHS pay scale cannot reach.
The realistic ceiling inside the NHS, without crossing into Director-level executive roles, is Band 8b. That is not a small ceiling. The ceiling outside the NHS, for a doctor with strong Clinical Safety credentials and a real track record, has not yet been mapped.
What to do this Week
Three things, in order, if this is the work you want.
Go to the NHS England Digital Clinical Safety training portal and enrol in the Foundation course. It is free, online, and takes between four and eight hours. Finish it this week. Then enrol in the Practitioner course. This is what The Christie’s job pack asks for as essential, and what almost every Digital CSO role in the dataset lists as a prerequisite.
Find three current Clinical Safety Officers on LinkedIn. One in an NHS trust, one in a health tech company, one in NHS England or an Integrated Care Board. Read everything they have written publicly in the last six months. Do not message them yet. You are learning the language and the texture of the work before you start using it.
Open the next safety incident in your own clinical area. Read it with new eyes, as if you were going to chair the post-incident review. Write down what you would ask, in what order, of whom, to understand what nearly went wrong. That note is the start of your portfolio for an interview.
The doctors who do well in this role are not the ones who memorised the regulations cold. They are the ones who could still hear about a near-miss and want to know, immediately, what nearly went wrong.
Cheers,
Dr. Ron
Join over 6000+ subscribers at Behind The Scenes in Health with Dr.Ron’s substack where we share insightful information around healthcare and health tech.
Help us grow on YouTube channel by subscribing, commenting and sharing as we post new videos every Friday by 7pm (WAT). Give us a follow on TikTok
If there are topics you would love to read about or guests you would like to see and hear on the podcast, please email me at ronald@mrimedic.com or podcast@mrimedic.com
Here is our linktree. Feel free to explore our pages.
Stay tuned for more inspiring stories and insights into the world of alternative careers. Subscribe to our blog for updates and join us on this journey where passion meets purpose.
The numbers in this piece come from Career Co-Pilot, the platform I built to track non-clinical NHS career intelligence. If you want the full breakdown of all six sub-tracks under Clinical Safety, including bands, employers, salaries and transition pathways, the role guide is at careercopilot.academy.